OverdoseFreePA Overdose Death Drug Review and Data Standardization
- Overview
Once a coroner or collaborator submits a case to OverdoseFreePA, the provided toxicology/ accompanying information is reviewed using the following protocol in order to best identify the drug(s) consumed.
- Reviewing the Toxicology of Drug-Related Overdose Deaths
-
- Initial Steps for Reviewing a Case
-
-
- Review toxicology report; identifying parent drugs and their metabolites. Only parent drugs or drugs consumed are identified on the public site and used by the website for analysis. However, all metabolites are retained in the database.
- Identify drugs that are not considered to be contributory to death and remove from the public database by unchecking the “contributory” box. Examples include:
- Caffeine
- Nicotine/Cotinine
- Theobromine
- Naloxone
- Review any additional information provided. Additional information can be used to determine the presence of heroin and other drugs with complex metabolic pathways. Information provided can include:
-
-
-
- Drug paraphernalia
- Prescription bottles
- Evidence of injection sites
- Overlapping prescriptions
- Presence of Naloxone
-
-
-
- Review provided demographic information, if components (ex. Age, race, etc.) are missing, contact the coroner/collaborator for more information.
- If there are questions regarding the case, drugs, or evidence, the coroner is contacted and makes the final decision.
- If there are multiple entries for one drug, create a parent drug using the source with the highest concentration and make the remaining sources metabolites.
-
-
- Reviewing Drugs Listed on Toxicology Reports
- Cannabinoids (SI Chart 1)
- Cannabinoids are metabolized into If 11 hydroxy-Delta THC, 11-nor-9-Carboxy-THC, Delta-9-THC, Delta-9-Carboxy THC or THC. When present, they should be made metabolites of cannabinoids.
- If cannabinoids are listed, then create a parent drug using the entry with the highest concentration.
- If cannabinoids are not listed on the toxicology report, create a “ghost parent” named cannabinoids and add any of the metabolites under new the cannabinoid parent, then uncheck the contributory box.
- Cocaine (SI Chart 2)
-
- Cocaine is metabolized into cocaethylene, benzoylecgonine, ecgonine methyl ester, and anhydroecgonine methyl ester. When present, they should be made metabolites of cocaine.
- If cocaine is listed, then create a parent drug using the highest concentration.
- If cocaine is not listed on the toxicology report in the presence of a metabolite, create a “ghost parent” named cocaine and add any of the metabolites under the new cocaine parent.
- Ethanol
-
- When blood alcohol concentration (or BAC) or whole blood ethanol are present, list as metabolites of ethanol.
-
- If ethanol is listed, then create a parent drug using the entry with the highest concentration.
- If ethanol is not listed on the toxicology report, create a “ghost parent” named ethanol and add any of the metabolites under the new ethanol parent.
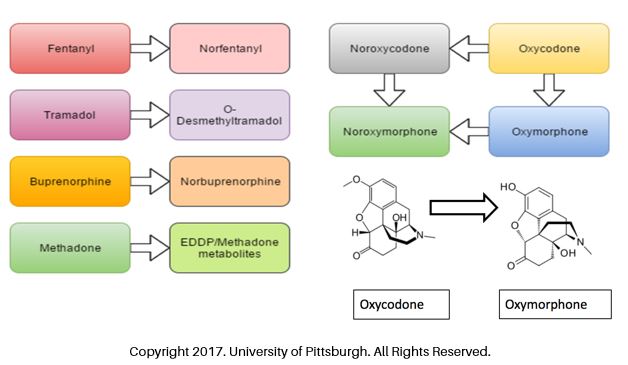
- Opioids and Synthetic Opioids (SI Charts 3 and 4)
-
-
- Fentanyl
-
-
-
- Fentanyl is metabolized into norfentanyl. When present, norfentanyl should be listed as a metabolite of fentanyl.
- If fentanyl is listed, then create a parent drug using the entry with the highest concentration.
- 4-ANPP is a precursor used in the creation of some fentanyl’s , when present it should be made a metabolite of fentanyl.
-
- If fentanyl is not listed on the toxicology report in the presence of a norfentanyl, create a “ghost parent” named fentanyl and add any of the metabolites under the new fentanyl parent.
- Non-Prescription Synthetic Opioids (NPSO)
-
- If a NPSO is listed, then create a parent drug using the entry with the highest concentration.
- 4-ANPP is a precursor used in the creation of some NPSO’s, when present it should be made a metabolite of a NPSO.
-
-
- Each NPSO should be listed as a separate parent drug.
- Heroin, Morphine, and Codeine
- Heroin is metabolized into 6-monoacetylmorphine, morphine, and codeine.
-
- If 6-monoacetylmorphine (6-MAM) is present, create a heroin ghost parent and add 6-MAM, morphine, and codeine as a metabolites.
- If morphine only is listed, then review the following information, to determine if the morphine is attributed to the consumption of heroin or pharmaceutical morphine. If the following information indicates the presence of morphine is more likely from the consumption of heroin, ask the coroner if the morphine is more likely heroin. If yes, list morphine as a metabolite of heroin. Information to review includes:
-
-
-
- Scene evidence of paraphernalia, stamp bags, tourniquets, syringes, etc.
-
-
-
-
-
- Presence of fentanyl in the same case
- If low levels of codeine are present, evidence is consistent with codeine being an impurity of heroin and should be made a metabolite of heroin.
-
-
-
-
-
-
- Higher levels of codeine and a codeine to morphine ratio of greater than 10:1 are most consistent with codeine as the parent drug, especially if supported by known prescription history and/or scene investigation.
-
-
-
- Prescription Opioids (SI Charts 3 and 4)
- Oxycodone
- Oxycodone is metabolized into oxymorphone and noroxycodone and should be made metabolites of oxycodone.
- If oxycodone only is listed, then create a parent drug using the entry with the highest concentration.
- If oxycodone and oxymorphone are both present, oxymorphone should be listed as a metabolite of oxycodone if the ratio is 0.28 or less (oxycodone to oxymorphone) between the two levels.
-
- Oxymorphone
-
- Oxymorphone is metabolized into noroxymorphone and should be made a metabolite of oxymorphone.
-
- If oxymorphone only is listed, the create a parent drug using the highest concentration.
-
-
- Hydrocodone
-
-
-
- Hydrocodone is metabolized into hydromorphone, norhydrocodone, and dihydrocodeine. When present, they should be made metabolites of hydrocodone, unless it follows an exception.
-
-
- If hydrocodone only is listed, then create a parent drug using the entry with the highest concentration.
-
- If hydrocodone and hydromorphone are both present, hydromorphone should be listed as a metabolite of hydrocodone if the level was significantly lower.
-
- Hydromorphone
- Hydromorphone is metabolized into Hydromorphone -3 -glucuronide, or Hydromorphic. When present, they should be made metabolites of hydromorphone.
- Hydromorphone
-
- If hydromorphone is listed, then create a parent drug using the entry with the highest concentration.
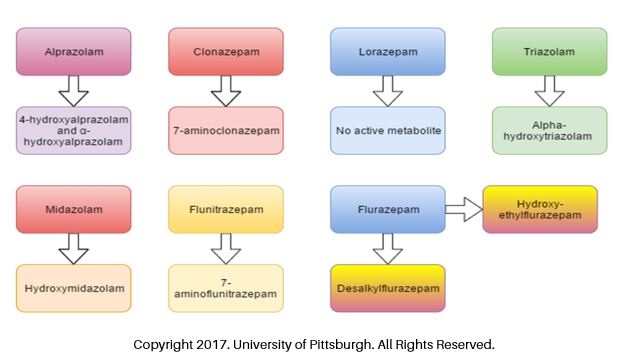
- f. Benzodiazepines (SI Charts 5 and 6)
-
- If the following parent and child drug combinations appear, make the appropriate match:
-
-
- Alprazolam and α-Hydroxyalprazolam
- Clonazepam and 7-Aminoclonazepam
- Midazolam and α –Hydroxymidazoalm
- Triazolam and α-Hydroxytriazolam
- Flurazepam and N-1-Desalkylflurazepam or N-1-Hydroxyethyl-Flurazepam
-
-
-
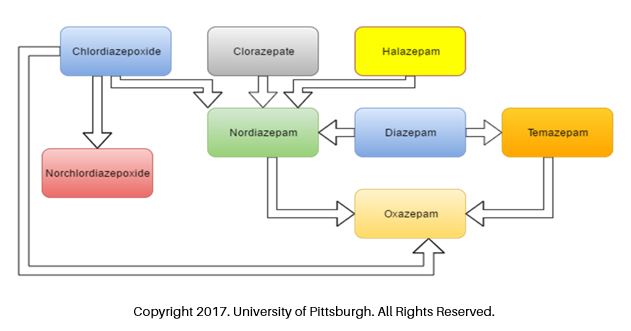
- Diazepam
- Diazepam is metabolized into nordiazepam, temazepam, and oxazepam. When present, they should be made metabolites of diazepma, unless it follows an exception.
- If diazepam is listed, then create a parent drug using the entry with the highest concentration, unless it follows an exception.
- Diazepam
-
-
-
-
- When nordiazepam is also present with low levels of temazepam and oxazepam, make diazepam the parent drug and add temazepam, oxazepam, and nordiazepam metabolites.
-
-
-
-
- Chlordiazepoxide
- Chlordiazepoxide is metabolized into desmethylchlordiazepoxide, demoxepam, nordiazepam and oxazepam. When present, they should be made metabolites of chlordiazepoxide, unless it follows an exception.
- If chlordiazepoxide is listed, then create a parent drug using the entry with the highest concentration, unless it follows an exception.
- Chlordiazepoxide
-
-
-
-
- If only desmethylchordiazepoxide or demoxepam are present, then make chlordiazepoxide the parent drug.
- If nordiazepam and oxazepam are also present, then classify as metabolites of chlordiazepoxide.
-
-
-
-
- Temazepam
- Temazepam is metabolized into oxazepam. When present oxazepam should be made a metabolite of temazepam, unless it follows an exception.
- Temazepam
-
-
- If temazepam is listed, then create a parent drug using the entry with the highest concentration, unless it follows an exception.
-
-
-
- If temazepam and oxazepam are present, in the absence of any other benzodiazepine metabolite, make temazepam the parent drug and oxazepam a metabolite.
-
-
-
-
- Nordiazepam
-
-
-
-
- In cases when the parent drug cannot be identified, nordiazepam is classified as the parent.
-
-
-
-
- Oxazepam
-
-
-
-
- Oxazepam does not have any active metabolites.
-
-
-
- If oxazepam is listed in the presence of no other benzodiazepines or metabolites, then create a parent drug using the entry with the highest concentration.
-
-
-
- Oxazepam in the presence of diazepam is classified as the metabolite of diazepam.
- Oxazepam in the presence of chlordiazepoxide, demoxepam, or desmethylchordiazepoxide is classified as metabolite of chlordiazepoxide.
- Oxazepam in the presence of temazepam (and no other benzodiazepines) is classified as metabolite temazepam.
-
-
- Amphetamines
-
-
- Amphetamine
- Amphetamine has no active metabolites.
- Amphetamine
- If amphetamine is listed, then create a parent drug using the entry with the highest concentration.
-
-
-
- Methamphetamine
- Methamphetamine is metabolized into amphetamine.
- Methamphetamine
- If methamphetamine is listed, then create a parent drug using the entry with the highest concentration, unless it follows an exception.
-
- If methamphetamine and amphetamine are both present, methamphetamine should be made a parent drug if the concentration is significantly higher than amphetamine. Amphetamine would then be listed as a child of methamphetamine.
-
-
-
-
- 3,4- Methylenedioxyamphetamine (MDA)
-
-
-
- MDA has no active metabolites.
- If MDA is listed, then create a parent drug using the entry with the highest concentration.
-
-
-
- 3,4-Methylenedioxymethamphetamine (MDMA, ecstasy)
- MDMA is metabolized into MDA, hydroxy-3-methoxyamphetamine (HMA), and 4-hydroxy-3-methoxymethamphetamine (HMMA).
- If MDMA is listed, then create a parent drug using the entry with the highest concentration.
- When MDA, HMMA, or HMA are present, they should be made a metabolite of MDMA.
- 3,4-Methylenedioxymethamphetamine (MDMA, ecstasy)
-
- If MDMA is not listed on the toxicology report in the presence of a MDAC, create a “ghost parent” named MDMA and add any of the metabolites under the new MDMA parent.
- Bath Salts
-
- If a Bath Salt is listed, then create a parent drug using the entry with the highest concentration.
-
-
- Each bath salt compound should be listed as a parent drug.
-
- Amitriptyline and Nortriptyline
-
-
-
- Amitriptyline is metabolized into nortriptyline; nortriptyline is an active metabolite.
-
-
-
- If amitiptyline is listed, then create a parent drug using the entry with the highest concentration.
- if the level of amitriptyline is significantly higher then list nortriptyline as a metabolite of amitriptyline.
- If nortriptyline is listed in the absence of amitriptyline, ask the coroner for more information.
- Citalopram/Escitlopram
-
-
- If citalopram, escitalopram, or citalopram/escitalopram are present, the entry with the highest concentration should be made a parent drug.
-
Key Terms:
Parent Drug – Parent drugs are the drugs that a person consumed prior to death. Parent drugs are what appear on the public site.
Child Drug – Child drugs, or metabolites, are the drugs that appear on the toxicology report and appear from the chemical breakdown of parent drugs by the body.
Ghost parent – A ghost parent drug is added when only a metabolite appears on a provided toxicology report/case submission. A reviewer will add in a blank drug entry that will be used in place of a traditional parent drug. Ghost parents have no associated levels and should only be added when the metabolite could have only come from the consumption of the specific drug.
Family Unit – A group of parent and child metabolites.
Relevant Manuscripts
- Edwards, H.T., Strenghening Forensic Science in the United States: A Path Forward. 2009, National Academy of Sciences.
- Davis, G.G., Complete republication: National Association of Medical Examiners position paper: Recommendations for the investigation, diagnosis, and certification of deaths related to opioid drugs. J Med Toxicol, 2014. 10(1): p. 100-6.
- Drummer, O.H., Postmortem toxicology of drugs of abuse. Forensic Sci Int, 2004. 142(2-3): p. 101-13.
- Lehrmann, E., et al., Postmortem diagnosis and toxicological validation of illicit substance use. Addict Biol, 2008. 13(1): p. 105-17.
- Reis, M., et al., Reference concentrations of antidepressants. A compilation of postmortem and therapeutic levels. J Anal Toxicol, 2007. 31(5): p. 254-64.
- Launiainen, T. and I. Ojanpera, Drug concentrations in post-mortem femoral blood compared with therapeutic concentrations in plasma. Drug Test Anal, 2014. 6(4): p. 308-16.
- Regenthal, R., et al., Drug levels: therapeutic and toxic serum/plasma concentrations of common drugs. J Clin Monit Comput, 1999. 15(7-8): p. 529-44.
- Martin Schulz, S.I.-B., Hilke Andresen, Therapeutic and toxic blood concentrations of nearly 1,000 drugs and other xenobiotics. Critical Care, 2012. 16(4).
- Ellis, A.D., et al., Identifying cases of heroin toxicity where 6-acetylmorphine (6-AM) is not detected by toxicological analyses. Forensic Sci Med Pathol, 2016. 12(3): p. 243-7.
- Harruff, R.C., Tracking the Opioid Drug Overdose Epidemic in King County, Washington Using and Improved Methadoogy for Certifying Heroin Related Deaths. Academic Forensic Pathology, 2015: p. 499-506.
- Mertz, K.J., J.K. Janssen, and K.E. Williams, Underrepresentation of heroin involvement in unintentional drug overdose deaths in Allegheny County, PA. J Forensic Sci, 2014. 59(6): p. 1583-5.
- Jennifer Sable, P., Recommendations and Lessons Learned for Improved Reporting of Drug Overdose Deaths on Death Certificates 2016, Council of State and Territorial Epidemiologists. p. 1-16.
Download the Data Standardization Protocol
SI Chart 1: Cannabinoids
SI Chart 2: Cocaine
SI Chart 3: Opioids
SI Chart 4: Synthetic Opioids
SI Chart 5: Benzodiazepines
SI Chart 6: Diazepam, Oxazepam, and Temazepam
Copy Right 2017. University of Pittsburgh. All Rights Reserved.